
The Dictatorship
Without insurance, immigrant patients may face unregulated ‘medical deportation’

ALLENTOWN, PA. (AP) — Junior Clase’s cluttered kitchen table paints a picture of his life in the United States. Scattered across it are bottles of deodorant and conditioner that he sends back to the Dominican Republic, a Spanish-language Bible and a plastic medical brace for his wife, Solibel Olaverria.
Olaverria began having intense headaches and vomiting five months after she joined her husband in the U.S. In the emergency room, she was diagnosed with a brain aneurysm; during surgery to stop it from rupturing, she suffered a stroke and was induced into a coma.
She left the couple’s Allentown row house in December 2022 and has yet to return. Clase worries she never will.
In February 2023, Clase said, hospital administrators suggested transporting his still-comatose wife to a facility back in the Dominican Republic – an option he refused.
“They told me that they could send her back to my country,” he said – even without his consent. “At that moment, she was missing a piece of her skull. … If they put her in an airplane or a helicopter, it was possible that she would die.”
Though the federal government is the only entity with the jurisdiction to remove people from the U.S., hospitals across the nation sometimes return uninsured noncitizen patients in need of long-term care to their countries of origin.
Advocates call this “medical deportation.” Hospitals and medical transport companies refer to it as “medical repatriation.” By either name, the practice exists in ethical and legal gray areas – without specific federal regulations, widespread public knowledge or a national tracking system.
Facing limited options for care, some immigrant patients and family members may voluntarily decide to continue treatment outside of the U.S. Other times, experts say, the process occurs without full consent.
Lori Nessel, a professor at Seton Hall University who supervised a 2012 report about medical repatriation, said the practice amounts to “private deportation.”
“They were essentially being deported,” she said, “but outside of the legal process for deportation, because there was no immigration court involved.”
While some foreign governments track these repatriations, data is inconsistent and doesn’t reflect whether patients wanted to return, felt they had no other option or were forced to leave.
Over the past two decades, academics, advocates and reporters have struggled to put a number on the phenomenon, which involves a tangled network of hospitals, air transport companies and consulates that work in different states and countries.
Since 2020, the Philadelphia-based Free Migration Project has tracked 19 cases of patients facing medical deportation, through referrals and a telephone hotline it runs. Six of those came in the first six months of 2025, from cities in Pennsylvania but also Florida, New Jersey and New York, according to Adrianna Torres-García, deputy director of the organization.
“We’ve had a higher volume of cases in the same span of time than any other given year,” Torres-García said. “It’s also more complex cases.”
Experts believe medical deportation happens more than tracking efforts account for, and some worry cases could now increase, given that the practice sits at the intersection of health care and immigration – two systems undergoing drastic change in the second Trump administration.
Early on, Olaverria was able to get treatment under a federal law that requires Medicare-participating hospitals to provide stabilizing care to anyone with an emergency condition, regardless of insurance, ability to pay or immigration status. Hospitals can then file for reimbursement through Emergency Medicaid.
But the tax and spending cut bill President Donald Trump signed in July significantly reduces how much the government will pay into Emergency Medicaid. The law also makes some immigrants, including refugees and asylees, ineligible for traditional Medicaid and Medicare.
Immigrants without legal status have long been ineligible for these programs, and even green card holders have to wait five years before they are eligible for Medicaid.
In effect, experts said, the changes will leave even more immigrants uninsured and provide less funding for emergency care if they need it.
“If immigrants are unable to get as much coverage, then they’re not going to be able to get as much care,” said Andrew Cohen, an attorney with Health Law Advocates, a public interest law firm in Boston. “That’s where medical deportations could really grow.”
The legal requirement to treat anyone with an emergency condition won’t go away, said Benjamin Sommers, a health policy researcher at Harvard University. But with the federal government paying less toward Emergency Medicaid, states could also decide to reduce how much funding goes to emergency care, shifting the burden to hospitals – or individuals.
Patients “get sent bills that they often can’t pay, that often are going to go to collections,” Sommers said, adding that some may even go bankrupt. “Sometimes we see hospitals diverting patients. … I think there’ll be more of that.”
Raymond Lahoud, a Pennsylvania lawyer who represents hospitals and health networks in cases related to immigration, said hospitals fulfill their obligations to treat all patients but often need to consider further options once those patients are stabilized.
“There comes a point where the hospital has done everything it medically could do, and now that person has to move on to their next step in rehabilitation or certain kinds of end-of-life care,” he said.
U.S. citizens might be discharged to other hospitals, long-term care facilities or their families. Noncitizens, with limited access to health insurance, might instead get sent to a facility in their country of origin.
Hospitals sometimes pay private medical transport companies to conduct repatriations and provide in-air care. These services routinely cost tens of thousands of dollars but may still be cheaper than long-term or indefinite care; in the U.S., inpatient hospital care cost an average of $3,132 per day in 2023, according to health policy research firm KFF.
“Unfortunately, it becomes a financial burden to the hospital,” said Craig Poliner, president of MedEscort, an Allentown-based medical air transport company that works with hospitals to facilitate medical repatriations.
Poliner insisted that MedEscort would never repatriate a patient without consent and said company officials work with hospitals to follow the American Medical Association’s discharge guidelines.
“The patients really do better in their own countries, in their own culture,” he said. “We’re not forcing anybody back. We convince them why we think it’s better. If we have the right approach, it usually resolves itself.”
However, advocates noted that immigration status, a lack of insurance, the injury or illness itself, unfamiliarity with the health care system and language barriers can hinder someone’s ability to give informed consent.
In 2013, John Sullivan, a social worker based in Tempe, Arizona, traveled to Mexico to study medical repatriation as part of a Fulbright scholarship. He interviewed patients who had been sent back, along with family members, health workers and Mexican officials.
Sullivan said the circumstances surrounding consent in some of those cases were “unclear.” “It was almost like migrants would describe feeling like they had no other choice,” he said.
Olaverria entered the U.S. on a temporary tourist visa, and when she sought treatment, she was uninsured. In the first days of March 2023, Clase said, hospital administrators gave him an ultimatum: Find care for his wife elsewhere, or they would follow through with her transfer to the Dominican Republic.
Clase said the only option he felt he had was to keep his wife where she was. He didn’t believe she would survive the flight to the Dominican Republic, and if she did, he didn’t trust that she’d receive the care she needed there. He couldn’t properly care for her at home, and she didn’t have insurance to cover the cost of another facility in the U.S.
Local advocates connected Clase with the Free Migration Project, which organized protests against Olaverria’s transfer. Outside the hospital, protesters carried homemade signs on neon-colored posters calling for an end to medical deportation.
After local media coverageClase said, hospital administrators agreed to hold off on the transfer if they could work together to find another long-term care option. The hospital did not respond to requests for comment.
Media coverage of Olaverria’s case helped bolster interest in a bill before the Philadelphia City Council to stop nonconsensual medical repatriations, and in December 2023, it became the nation’s first and only law banning the practice, according to experts.
The policy requires hospitals in the city to obtain patients’ written consent and provide information about their rights and options for care before transferring them out of the U.S. It also requires hospitals to determine whether patients are eligible for programs that could pay for their care – and, if so, help them enroll.
Philadelphia hospitals also must now report medical repatriations to the city’s Department of Public Health. Agency spokesman James Garrow said hospitals submitted five repatriation reports in 2024, the first full calendar year for which data was collected.
Claudia Martínez participated in the campaign to pass the law after her uncle faced medical repatriation. The personal photos, wedding memorabilia and Bible quotes that decorate her living room walls hang alongside a “Community Power Award” from the Pennsylvania Immigration Coalition.
“I don’t want anyone to go through what I went through,” Martínez said.
In May 2020, a motorcycle struck Martínez’s uncle, an immigrant from Guatemala. When Martínez arrived at the hospital, she found him comatose and intubated, with injuries that rendered him almost unrecognizable.
Weeks later, Martínez said, a hospital social worker asked for her uncle’s immigration status. She later learned the hospital and MedEscort planned to transfer him to a facility in Guatemala.
“I was in shock,” Martínez said. “He was intubated. … He was not in a condition to travel.”
She said she rejected the transfer in conversations with hospital officials and MedEscort, but Poliner said MedEscort got authorization for the repatriation from family members in Guatemala. Martínez disputes that.
Eventually, Martínez connected with the Free Migration Project, which organized a protest outside the hospital on the day of her uncle’s scheduled trans fer.
In the end, the medical deportation was scrapped. Ultimately, with the help of community advocates, Martinez’s uncle was able to access a form of state-sponsored insurance. He moved into a rehabilitation center and stayed for three years, until his insurance ran out.
In May 2024, his family decided it would be best for him to return to Guatemala to be at home with his wife. He can walk again but has significant memory impairments.
“He is someone who loves to joke,” Martínez said. “This, I think he didn’t lose.”
Consulates are often involved in the medical transport of their citizens, helping to secure travel documents and occasionally paying for airfare on less expensive commercial flights.
Between 2014 and 2024, the Mexican General Directorate of Consular Protection and Strategic Planning reported 8,227 medical repatriations; 328 of those took place in 2024. The data does not distinguish between patients who wanted to return and those who felt pressured or coerced.
“Sometimes the level of care that they are going to receive in their hometowns … is not going to compare to the one they receive here, and they know that – so it’s very rare that a patient says, ‘I want to leave,’” said one Mexican consular official, who did not want to be named to avoid repercussions in their ongoing work with hospitals.
If patients want to stay in the U.S., they may not know what options are available to them. Hospitals, too, may be unaware of alternatives, said Cohen, who runs a program that helps eligible immigrant patients access insurance.
In some states, immigrants who don’t qualify for federal insurance programs may be able to access certain state-funded programs instead.
“(Hospitals are) preemptively doing something that they wouldn’t even need to do if they knew about these pathways into better coverage,” Cohen said.
In May 2023, Olaverria was transferred into a long-term care facility in Allentown. Two months later, she woke up from the coma. She still cannot walk or use the bathroom on her own, and she can speak only a few words.
Later that year, Clase and his wife obtained medical deferred action, which allowed them to temporarily remain in the country. It also allowed Clase to get a work permit and Olaverria to access emergency medical assistance from the state.
Between working two jobs and attending church services three times a week, Clase keeps his ritual of visiting his wife every day. Flower bouquets rest on the bookshelf in her room.
He wipes her mouth, adjusts her neck and massages her curled-in hands. And he still tells her stories that can make her laugh.
For him, life outside this routine is virtually nonexistent. When he gets home each night, he sleeps and occasionally cries.
“This country consumes you,” he said.
Clase and Olaverria are working to apply for a visa that would allow them to stay longer. But her ability to continue in long-term care is uncertain.
Despite this, Clase carries forward, focused on the familiar paths of his daily routine, all of which lead to Olaverria.
“The majority of my time,” he said, “I dedicate it to my wife.”
___
This report is part of “Upheaval Across America,” an examination of immigration enforcement under the second Trump administration produced by Carnegie-Knight News21. For more stories, visit https://upheaval.news21.com/


After a chemical leak at the Ames Goldsmith plant in Kanawha County killed two workers and injured dozens more last month, federal investigators quickly arrived in West Virginia to begin piecing together what went wrong.
Now, the federal agency tasked with determining the root cause of the accident could be eliminated.
President Trump is proposing to cut funding for the Chemical Safety and Hazard Investigation Board, a small federal agency that probes chemical disasters and pushes for safety fixes.
Worker advocates and former CSB members warn dismantling the agency could leave states like West Virginia — with long histories of deadly industrial chemical incidents — more vulnerable to future disasters.
The board has opened investigations into eight chemical incidents in West Virginia since 2008.
Maya Nye, federal policy director for the environmental health organization Coming Clean, said before the most recent chemical leak at the Ames Goldsmith plant, the 2008 explosion at the Bayer Crop Science plant in Institute was the deadliest in her recent memory. Two workers were killed in that incident as well.
“These can be prevented,” she said. “Every incident that occurs is 100% preventable.”
Many of the state’s chemical facilities are concentrated along the Kanawha Valley’s industrial corridor.
Those incidents include a toxic release at DuPont’s Belle plant in 2010 that killed a worker. And in 2014, a spill at Freedom Industries tainted the drinking water of hundreds of thousands of people.
Advocates say the impacts of chemical incidents often extend far beyond plant workers.
Nye said low-income communities and communities of color often face the greatest risks. But the employees stand to lose the most.
“Workers are typically hurt first and worst,” she said.
Why the Chemical Safety Board matters
The White House said the CSB duplicates work already done by the Environmental Protection Agency and the Occupational Safety and Health Administration and argued that eliminating it would help shrink the federal government.
But Congress created the board after growing frustration that existing federal agencies were not adequately investigating major industrial chemical disasters.
The safety board was created through amendments to the Clean Air Act in 1990, and has a budget of around $14 million and fewer than 50 employees. It was modeled after the National Transportation Safety Board, which investigates airplane and train crashes.
Jordan Barab, a former deputy assistant secretary at OSHA, said the CSB investigates industrial chemical incidents differently than enforcement agencies.
While OSHA and the EPA primarily determine whether companies violated existing regulations, Barab said the board conducts broader “root cause” investigations into why disasters happened in the first place.
“They can look at other problems, other causes that aren’t necessarily covered by regulations or standards,” he said.
The CSB can unearth problems like worker fatigue, lack of routine maintenance, management changes and broader safety culture problems inside facilities, he said.
After the release of toxic chemicals at DuPont’s Belle plant in 2010, board investigators determined that a lack of planning and a lack of communication between plant operators, as well as deferred maintenance, had caused the leak.
The CSB has issued more than 1,000 recommendations over its history, many of which were later adopted by companies, trade associations and state regulators.
“A lot of the ways the industry has modernized to improve safety are based on recommendations that came out of the CSB,” Barab said.
The board has also publicly criticized recent efforts by the Trump administration to roll back chemical safety regulations known as Risk Management Program rules.
Earlier this year, the board warned the rollback would represent “a significant step backwards” in preventing catastrophic chemical accidents.
Trump proposes cuts to multiple worker protection agencies
The Trump administration has proposed eliminating the board multiple times in the past.
Rick Engler, a former CSB member appointed by President Barack Obama, said Congress has repeatedly rejected past attempts to eliminate the agency.
Despite its size, Engler said eliminating the board would leave a major gap in federal chemical safety oversight.
“It’s a very small agency,” he said. “But without the CSB, preventative solutions will not be identified.”
Kelly Moore, a spokesperson for Sen. Shelley Moore Capito, R-W.Va., said the senator has long supported the CSB and voted in the past to support additional funding for the agency.
Moore did not answer if Capito would support President Trump’s cuts this year.
The potential loss of the agency comes as federal workplace safety agencies already face staffing shortages and proposed budget cuts.
The Trump administration has proposed cuts to other agencies that protect workers. He proposed a 7.5% cut to OSHA’s budget and a 10% cut to the federal mine safety agency’s budget.
Barab said the administration’s push to eliminate the agency is especially puzzling because the board largely provides the kind of safety guidance and recommendations that Trump officials have said they prefer over aggressive enforcement.
“It’s ironic,” he said, “that they should try to kill an agency that actually does exactly that.”
___
This story was originally published by Mountain State Spotlight and distributed through a partnership with The Associated Press.
The Dictatorship
Trump administration pushes for 25% tariff on Brazil after US Supreme Court shot down last attempt

WASHINGTON (AP) — The Trump administration proposed 25% tariffs on imports from Brazilcharging that the world’s 10th-biggest economy engages in trade practices that are “unreasonable’’ and that “burden or restrict U.S. commerce.’’
Brazil’s President Luiz Inácio Lula da Silva said he received the decision “with indignation.” He also blamed the decision by the U.S. administration on his rival in October’s elections, Sen. Flávio Bolsonaro, who visited Washington last week. The senator is the son of former President Jair Bolsonaro, once nicknamed “the Trump of the Tropics” by his allies.
The announcement late Monday came after an investigation by the Office of the U.S. Trade Representative, charging Brazil with lax anti-corruption enforcement and unfair tariffs of its own, among other things.
The U.S. has had a goods trade surplus with Brazil for years.
U.S Trade Representative Jamieson Greer said that he and President Donald Trump had “constructive’’ meetings with Lula and other Brazilian officials. But he said that “we continue to have substantial differences in resolving the issues identified in this investigation.’’
Lula on Tuesday cited other reasons for the punishing tariff proposal. For the first time he named an American official as a hurdle to his relations with Trump and once again he threatened to retaliate.
“I spoke to President Trump for three hours, and that Marco Rubio guy, the head of the State Department, he is anti-Latin American,” Lula said. “He is a deadly enemy of Cuba, a deadly enemy of many Latin American countries. I already told Trump that he does not like Brazil.”
The U.S. State Department did not immediately respond a request for comment from The Associated Press on Tuesday.
Brazil’s government said in a statement that its dialogue with American counterparts, which includes “personal involvement of Presidents Lula and Trump,” is being ”sabotaged by merely electoral and family matters” of the Bolsonaros.
It added that it hopes “the recommendations do not become effective tariffs.”
“But we stress we will adopt every measure that is capable of reducing the damage that might be caused to the national economy, to the jobs and the income of Brazilians,” the country’s government said.
Last year, Trump had slapped Brazil with a 50% tariff, mainly to protest its prosecution of Jair Bolsonaro for trying to overturn his electoral defeat in 2022. Trump’s relationship with Lula seemed to have improved early May, when the Brazilian visited the White House.
But last week, the Trump administration designated two Brazilian gangs as terrorist organizationsafter Sen. Bolsonaro’s visit. Lula opposes the designation, which analysts say could bolster his political rival.
Sen. Bolsonaro published in his social media channels a statement he said he sent to Rubio, in which he criticizes the potential new tariff hike for it would cause “serious damages to the Brazilian people — precisely the citizens that see the United States as a partner and a friend.”
“I am writing to formally repeat the request I did to you in person, that the U.S. do not impose tariffs on Brazil,” Sen. Bolsonaro said.
Greer’s office has scheduled a public hearing July 6 on the proposed tariffs.
Trade lawyer Ryan Majerus, a partner at King & Spalding, noted said that the administration’s plan excludes more than half of U.S. imports from Brazil, including aircraft and key minerals.
The Trump administration invoked Section 301 of the Trade Act of 1974 to launch the investigation into Brazil’s trade practices.
Sen. Bolsonaro travelled to meet officials in Washington last week in the wake of a scandal at home in which he admitted receiving funds from a disgraced banker. Another son, former lawmaker Eduardo Bolsonaro, was also present.
On Tuesday, Trump posted a photo of the Bolsonaros in the Oval office on his social media site.
“These sons of Bolsonaro can be worse than him. They are actually sellouts of our country, they went there to ask a foreign nation to meddle in Brazilian affairs,” Lula said in a speech to residents of the city of Catalao, south of capital Brasilia. “They are traitors.”
The U.S. Supreme Court ruled in February that Trump overstepped his authority by using a different law – the International Emergency Economic Powers Act (IEEPA) of 1977 – to impose sweeping tariffs on U.S. trading partners, including Brazil.
However, Section 301 tariffs have survived legal challenges, and the administration is likely to use that authority to impose other tariffs and to recoup some of the tax revenue lost when the Supreme Court rejected the IEEPA tariffs.
Brazil’s president said that during his visit to Washington early May, he handed Trump documents showing that the U.S. has a trade surplus with Brazil.
Documents published by the U.S. Trade Representative show that last year, U.S. exports to Brazil rose nearly 11% to $54.4 billion. Brazilian exports to the U.S. fell 5.7% to $39.9 billion, meaning the U.S. had a trade surplus of more than $14 billion.
The trade imbalance for services is more lopsided in favor of the U.S., with services exports in 2024 reaching $29.6 billion, quadruple the Brazilian services exports to the U.S.
“I am not going to cry about it,” Lula said. “If they (the U.S.) don’t want to buy from us, we will sell to someone else.”
China has been Brazil’s biggest trading partner for about a decade.
____
Mauricio Savarese reported from Sao Paulo.
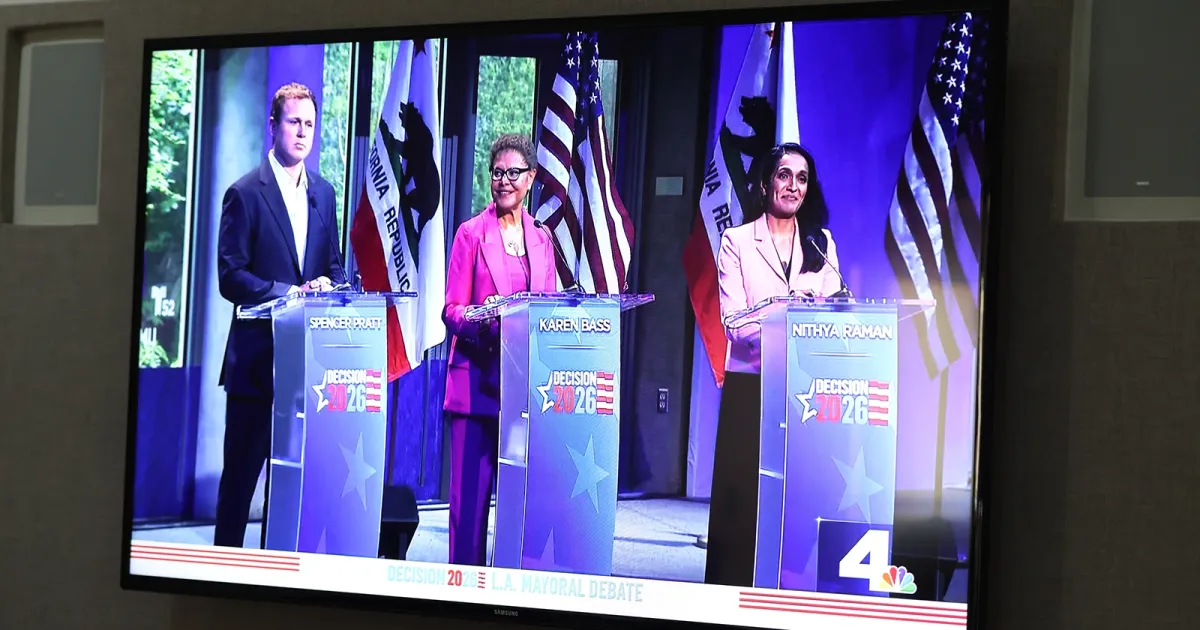
Incumbent mayor Karen Bass will proceed to the Nov. 3 general election in the Los Angeles mayoral race, the Associated Press projected early Wednesday morning.
Bass emerged as the leader of the crowded field of more than a dozen candidates after a feisty battle the past few months that led to former reality TV star Spencer Pratt and Los Angeles City Councilwoman Nithya Raman polling neck-and-neck less than a week before primary day.
As of early Wednesday morning, the Associated Press had yet to project a second candidate who would advance to the general election in the all-party primary in which the top two vote-getters move on.
Bass, the 72-year-old incumbent, has a long record in politics: Before being elected LA mayor in 2022, she represented Los Angeles in the California State Assembly, eventually becoming speaker, and served six terms in the U.S. House of Representatives. She entered the mayor’s race facing extensive criticism from Angelenos for both her handling of last year’s deadly LA wildfires — she was in Ghana when the blazes broke out — and her failure to achieve her goal of ending homelessness by the end of her first term.
Bass has campaigned on her experience, which includes standing up to the Trump administration when the president deployed Immigration and Customs Enforcement to the city last year, and a pledge to deliver on her promise to end homelessness.
Pratt, 42, was a surprise candidate when he announced his intention to run for mayor in January. The registered Republican and former reality TV villainbest known from the MTV show “The Hills,” has no political experience, but became a vocal critic of Bass and Democratic Gov. Gavin Newsom after his family home burned down in the Pacific Palisades fire last year. Since launching his populist campaign centered on critiquing the city’s Democratic leadership and cracking down on homelessness and crime, Pratt has earned the backing of MAGA leadersand even President Donald Trump himself, though Pratt rejects any affiliation with the MAGA movement.
After a strong televised debate performance last month, Pratt’s fundraising surged. All in all, he has raised $3.7 million since January, compared to the $3.2 million Bass has raised over the past two years, according to the latest campaign finance filings.
Raman, a member of the Democratic Socialists of America who has represented LA’s 4th council district since 2020, launched her surprise mayoral campaign in February — less than two weeks after she endorsed Bass’ campaign for re-election.
Raman, 44, earned comparisons early on to New York City Mayor Zohran Mamdani due to her DSA roots and her pledge to bring generational change to the city if elected. But as the race progressed, she walked back some of her more left-wing policy stances — such as defunding the police and opposing anti-camping zones for homeless people — and polling suggested Raman and Pratt would be fighting for second place on primary day.
This is a developing story. Check back for updates.
Julianne McShane is a breaking news reporter for MS NOW who also covers the politics of abortion and reproductive rights. You can send her tips from a non-work device on Signal at jmcshane.19 or follow her on X or Bluesky.
- Georgia Republicans want Trump’s endorsement — before it’s too late
- A judge said the Trump administration can’t dismantle a weather research center. The damage may already be done.
- House votes to halt Iran war in stinging loss for Trump
- Senate Republicans manage to unstick immigration funding bill
- She hired investigators to track her opponent

- Trump administration wants to cut agency that investigates chemical disasters

- Trump administration pushes for 25% tariff on Brazil after US Supreme Court shot down last attempt

- Mullin keeps door open to pull customs agents from ‘sanctuary city’ airports
- Mamdani makes big political gamble in backing Espaillat challenger

- Negotiators aiming to unveil draft of bipartisan House AI bill by week’s end
-

 Politics1 year ago
Politics1 year agoFormer ‘Squad’ members launching ‘Bowman and Bush’ YouTube show
-

 The Dictatorship1 year ago
The Dictatorship1 year agoLuigi Mangione acknowledges public support in first official statement since arrest
-

 Politics1 year ago
Politics1 year agoFormer Kentucky AG Daniel Cameron launches Senate bid
-
Uncategorized2 years ago
Bob Good to step down as Freedom Caucus chair this week
-
 The Dictatorship1 year ago
The Dictatorship1 year agoPete Hegseth’s tenure at the Pentagon goes from bad to worse
-

 The Josh Fourrier Show2 years ago
The Josh Fourrier Show2 years agoDOOMSDAY: Trump won, now what?
-

 Politics1 year ago
Politics1 year agoBlue Light News’s Editorial Director Ryan Hutchins speaks at Blue Light News’s 2025 Governors Summit
-

 The Dictatorship9 months ago
The Dictatorship9 months agoMike Johnson sums up the GOP’s arrogant position on military occupation with two words